
There are different ways to maintain and care for the type of urinary reconstruction you may undergo. It is important to communicate any questions or concerns you may have to your health care team. To learn more information or hear from patients who have undergone urinary reconstruction, visit the Bladder Cancer Advocacy Network (BCAN) website.
If you need to have your bladder removed, your surgeon will talk to you about your options for reconstructing and redirecting your urinary tract. There are three options:
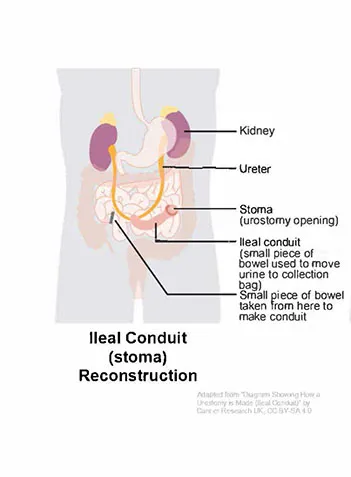
1. Ileal Conduit (Stoma)
A stoma, which is an opening at your skin. It is the shortest surgery and has the fastest rehab time, and your urine will drain into an external bag. This option is also called an ileal conduit.
_CRUK_124.svg){kind=link}
Caring for Your Ileal Conduit
If you had an ileal conduit urinary reconstruction (stoma with external collecting bag), you should receive special instructions from a Wound Ostomy Nurse on caring for your stoma and attaching your bag. There are different types of bags. You may want to sample different bag systems to see what works best for you. Know that your stoma will shrink until about 8 weeks after surgery. The bag system that works right away may not work as well in a month or two. Your health care team will teach you how to:
- Attach, detach, empty, and replace your bag system
- Use a nighttime drainage system and/or a leg bag
- Care for your stoma and the skin surrounding it
Tips for Caring for Your Ileal Conduit:
- Drink water daily to keep hydrated and keep the mucous made by the conduit flowing. (Remember, it used to be part of your intestines, so making mucous is natural.)
- Get support from other “urostomates” at www.bcan.org and www.ostomy.org.
- You can shower, swim, exercise, travel, and be intimate with the bag attached. There are also products you can purchase that help conceal or cover the bags.
- You must carry extra supplies with you at all times.
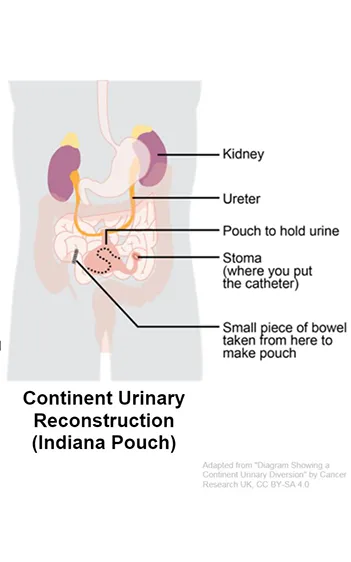
2. Continent Cutaneous Reservoir
A continent cutaneous reservoir, also known as a Koch or an Indiana pouch. This is a longer surgery that creates an internal bladder substitute with a stoma. You will manually empty the bladder reservoir using a catheter, about 6 or 7 times a day.
{kind=link}
Caring For Your Continent Cutaneous Reservoir
If you had a continent cutaneous reservoir (Koch or Indiana pouch), your health care team will teach you how to insert a catheter (a thin tube) into your stoma and drain urine from your internal pouch.
Tips for Caring for Your Continent Cutaneous Reservoir:
- Drink water daily to keep hydrated and keep the mucous made by the pouch flowing. (Remember, it used to be part of your intestines, so making mucous is natural.)
- Get support from other people with urostomies at www.bcan.org and www.ostomy.org.
- You must drain your pouch at least 4 or 5 times a day using a catheter. You will want to set an alarm at night so it is emptied every 4-6 hours. At first, you may be asked to drain the pouch every 2 hours.
- You must carry extra clean catheters with you at all times.
- Consider wearing a medical alert bracelet or including this information in your emergency health information on your smartphone.
Your treatment team will want to see you regularly to make sure your urinary reconstruction is working well. These appointments could include:
- Urine tests to check for infection
- Checking how well your kidneys are functioning.
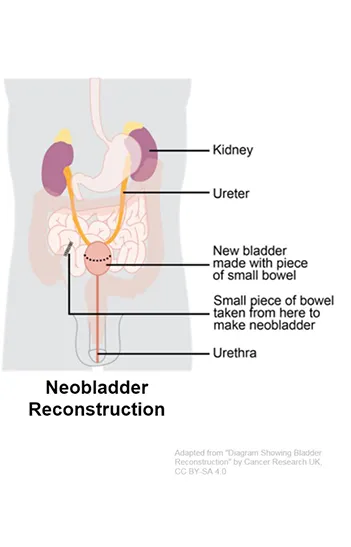
3. Neobladder
A neobladder. In this surgery, an internal bladder substitute is created and connected to your urethra, which allows you to urinate much as you did before. It is the longest surgery, and your recover will include learning how to use your abdominal muscles to urinate.
{kind=link}
Caring for Your Neobladder
If you had neobladder surgery, your surgeons created a “new bladder” which will take time to learn how to use. It can take time for your new bladder to stretch to a normal size and for the muscles that you are using to urinate to get stronger. You can expect:
- To wear adult diapers and incontinence pads as needed, at least at first
- Daytime incontinence to decrease three to six months after surgery
- Nighttime incontinence to decrease slowly over the first year after surgery
- Voiding to work differently. Your health care team will show you how to use different muscles to help empty your neobladder.
Tips for Caring for Your Neobladder:
- Drink water daily to keep hydrated and keep the mucous made by the neobladder flowing. (Remember, it is made out of pieces of intestines, so it is natural for it to make mucous.)
- Get support from other people with neobladders at www.bcan.org.
- You must urinate at least every 3-4 hours. You will need to set an alarm at night so you don’t go longer than 4 hours. You may also want to limit caffeine and fluids 3 hours prior to bedtime, so you only need to get up once during the night.
- Learn how to do Kegel/pelvic floor muscle exercises correctly and do them daily.
- Watch for stronger smelling or darker colored urine, which may signal a UTI. If you think you have a UTI, contact your health care team.
- Wear a medical alert bracelet and/or include this information in your emergency health information on your smartphone.
Your treatment team will want to see you regularly to make sure your new bladder is working well. These appointments could include:
- Urine tests to check for infection
- Checking how well your kidneys are functioning
- Assessing how well you can control urination
- Making fixes that can help you better control urination